Issue:
110
Page: 50-61
Artemisinin: A Nobel Prize-Winning Antimalarial from Traditional Chinese Medicine
by Connor Yearsley
HerbalGram.
2016; American Botanical Council
Half of the 2015
Nobel Prize in Physiology or Medicine was awarded to Chinese phytochemist Tu
Youyou for her role in the discovery of the natural compound artemisinin, which
is produced by the traditional Chinese medicinal herb qinghao (Artemisia
annua, Asteraceae), also known as sweet wormwood. Artemisinin derivatives
are commonly used in the treatment of malaria, one of the world’s oldest and
deadliest diseases.1-3
The other half
of the Prize was awarded to Japanese microbiologist Satoshi Ōmura, PhD, and
Irish-American biologist and parasitologist William C. Campbell, PhD, for their
discovery of avermectin, a natural anthelmintic compound (i.e., one that expels
worms and other parasites from the body). Avermectin is produced by the
bacterium Streptomyces avermitilis, and its derivatives have
dramatically reduced the incidences of parasite-induced diseases, such as river
blindness and lymphatic filariasis.3
Both halves of
the Prize are a triumph for the field of pharmacognosy (the study of medicines
derived from plants and other natural sources) and, according to many, Tu’s
half is also a win for China. Tu, who was born in 1930 in Ningbo, a port city
in Zhejiang province on the eastern coast of China, is the first citizen of the
People’s Republic of China (PRC) to be awarded a Nobel Prize in the sciences.
(Five Chinese-born scientists have won the Nobel Prize in Physics, but none
were citizens of the PRC.1) Some people in China view the win as
confirmation of the strength of Chinese science and medicine, while some
traditionalists view it as a reminder that Chinese medicine is ignoring its
heritage by using methods similar to those used by Western pharmaceutical
companies.4
In truth, the
discovery of artemisinin, which also involved ethnobotany, the study of
people’s historical uses of plants, may be a prime example of traditional
Chinese medicine (TCM) and Western practices complementing each other.
The discovery
of artemisinin is considered one of the most important advancements in the
treatment of malaria since the isolation of quinine in 1820. Quinine is a
natural compound found in the bark of South American trees in the genus Cinchona
(e.g., C. officinalis, Rubiaceae). These trees are native to the
rainforests of the Andes Mountains, and extracts of their bark had been used to
treat fevers caused by malaria at least as far back as 1632.2,5-7
Artemisinin
derivatives are the most effective of all current antimalarial drugs.8
In April 2001, the World Health Organization (WHO), which directs and
coordinates international health within the United Nations (UN) system, first
recommended the use of artemisinin-based combination therapies (ACTs), which
combine an artemisinin derivative with another, longer-lasting antimalarial
drug.9 Since then, ACTs have saved millions of lives.10
History of
Artemisinin
The discovery
of artemisinin can be traced back to 1967, during the tumult of the Chinese
Cultural Revolution, when many Western-trained Chinese scientists were being
persecuted by the Communist Party. At the same time, the Vietnam War was
escalating, and many North Vietnamese soldiers were falling victim to malaria
that had developed resistance to chloroquine (a synthetic analog of quinine)
and other drugs.1,11 Communist North Vietnam, an ally to China,
asked for China’s help to find a new treatment for malaria, which was also
afflicting many people in southern China, as well as thousands of American
soldiers who were fighting against North Vietnam. (The US Department of Defense
undertook its own drug hunt, which eventually produced mefloquine, another
synthetic analog of quinine.)1,2,11
In response to
North Vietnamese President Ho Chi Minh’s appeal, Chinese Premier Zhou Enlai and
Chairman Mao Zedong set up a secret military project called Project 523
(because of its starting date, May 23, 1967) to find a solution. Progress was
slow at first, despite the fact that the initiative reportedly involved the
efforts of about 500 scientists working at about 60 laboratories and institutes
in China.1,12 Though the project was kept covert, and some details
of its history remain foggy even now, information flowed freely at joint
meetings among the different research groups involved. Three new malaria
treatments were produced by 1969.
Until the late
1960s, according to one source, the antimalarial remedy of choice in China,
perhaps by default, was changshan. The term “changshan” generally refers
to the root of Dichroa febrifuga (Hydrangeaceae), rather than to the
complex mixture that traditionally contained the root as a central component.
Changshan was mentioned in the Canon of the Divine Husbandman’s Materia
Medica, which was written circa 200 CE, as a treatment for fevers. However,
changshan has an intense emetic effect, which is compounded when the
active alkaloids are used in isolation from the rest of the plant, and when the
plant itself is used without the offsetting effects of the other ingredients
traditionally used in the mixture (e.g., ginger [Zingiber officinale,
Zingiberaceae], licorice [Glycyrrhiza glabra, Fabaceae], and betel nut [Areca
catechu, Arecaceae]). This effect led to the eventual disuse of drugs
derived from the root, and perhaps further necessitated the finding of a new, more
palatable treatment option.13
Tu, who
graduated from the Beijing Medical University School of Pharmacy in 1955 (she
has no postgraduate degree or research experience abroad, neither of which was
possible during the Cultural Revolution), did not become involved with Project
523 until January 21, 1969 when she was sent to Hainan Island off the southern
coast of mainland China. Tu, 38 at the time, was working at the Academy of
Traditional Chinese Medicine in Beijing when she was given the daunting task of
searching nature for a new malaria treatment.
“The work was
the top priority so I was certainly willing to sacrifice my personal life,” Tu
told New Scientist in 2011. While on the island, Tu observed
firsthand the toll malaria was taking on the population, and this was the
beginning of a decade of work.1,10 “I saw a lot of children who were
in the latest stages of malaria,” she said. “Those kids died very quickly.”
Tu also
visited TCM practitioners across China and compiled a notebook: “A Collection
of Single Practical Prescriptions for Anti-Malaria.”1 Back in
Beijing, Tu and her team investigated more than 2,000 traditional Chinese
herbal preparations.10 According to a 2011 written account by Tu,
her team “identified 640 hits that had possible antimalarial activities. More
than 380 extracts obtained from [about] 200 Chinese herbs were evaluated
against a mouse model of malaria. However, progress was not smooth, and no
significant results emerged easily.”29
According to
the same account, the turning point came when an extract of A. annua, or
qinghao, initially “showed a promising degree of inhibition against
parasite growth.” But this observation was not reproducible in subsequent
experiments. Tu and her team scoured the TCM literature looking for a possible
explanation and found one in physician Ge Hong’s medical text A Handbook of
Prescriptions for Emergencies, which was written circa 340 CE (some sources
say the text is called Emergency Prescriptions Kept Up One’s Sleeve).29,30
One passage in the text described a method of preparing qinghao to be
used for the treatment of “intermittent fevers,” one of the most telltale
symptoms of malaria. The passage reads: “qinghao, one bunch, take two sheng of
water [about two liters] for soaking it, wring it out, take the juice, ingest
it in its entirety.”30
Interestingly,
the text 52 Prescriptions contains the earliest known mention of qinghao
being used as a treatment, but in this case for hemorrhoids. The text was
compiled sometime between 1065 and 771 BCE, but it was sealed in a tomb in 168
BCE and was not discovered until 1973 (shortly after artemisinin was
discovered), during the excavation of the Mawangdui archeological site in
Changsha, Hunan, China.8,31 The earliest known mention of qinghao
being used to treat a disease resembling malaria is contained in Zhang Ji’s
text On Cold Damage, which dates to about the second century CE. The
text recommends treating “fevers with sweating and jaundice” with a mixture
containing boiled qinghao.8
Ge’s
instructions to take a juice wrung out of the entire fresh plant (rather than
an herbal tea prepared by pouring hot water onto dried plant material) probably
resulted in an emulsion of water, flavonoids, and aromatic oils, with higher
quantities of artemisinin than some other methods recorded in the Chinese
literature.30 These instructions also gave Tu the idea that the
heating involved with their original extraction method was probably destroying
the primary active components of the plant.29,30 “Indeed, we
obtained much better activity after switching to a lower temperature
procedure,” Tu wrote.29 This method was similar to the method Ge
described, but involved diethyl ether as the solvent.30 Organic
solvents (i.e., solvents that contain carbon), such as diethyl ether, generally
are better-suited for extracting hydrophobic compounds (i.e., compounds that
are not soluble in water), such as artemisinin. Diethyl ether, however, is
highly flammable.32
Tu wrote that
they separated the extract into its acidic and neutral portions, and that, on
October 4, 1971, they obtained a nontoxic, neutral (pH of 7) extract that
proved to be 100% effective when administered orally to mice that had malaria
caused by parasites of the species Plasmodium berghei and monkeys with
malaria caused by P. cynomolgi.
“During the
Cultural Revolution, there were no practical ways to perform clinical trials of
new drugs. So, in order to help patients with malaria, my colleagues and I
bravely volunteered to be the first people to take the extract,” Tu wrote.
After personally confirming the safety of the extract, Tu went back to Hainan
Island with her team to test its efficacy in patients infected with both P.
vivax and P. falciparum. “These clinical trials produced encouraging
results: patients treated with the extract experienced rapid disappearance of
symptoms — namely fever and number of parasites in the blood — whereas patients
receiving chloroquine did not,” she wrote.29
“We had just
cured drug-resistant malaria,” Tu told New Scientist. “We were very
excited.”1
In 1972, Tu
and her team identified a colorless, crystalline substance as the active
component of the extract, and named it qinghaosu (artemisinin).29
Artemisinin, whose structure was determined in 1975, is most abundant in the
leaves of A. annua, but the compound has also been found in other
species of Artemisia: A. apiacea and A. lancea, and in
small quantities in A. sieberi and A. scoparia.30,33
In fact, in polymath Shen Gua’s Dream Pool Essays, written in 1086 CE,
it is suggested that A. apiacea, not A. annua, was the species
the Chinese literature intended when referring to qinghao. A passage in
the text reads: “In the depth of autumn, when the other hao are yellow, this
one [A. apiacea] alone is blue-green; its smell is quite aromatic. I
guess [this is] the one the ancients used, they considered this one the
preferred one.” For this reason, it has been suggested that the name qinghao
(“blue-green hao”) should be reserved for A. apiacea and that huanghauhao
(“yellow blossom hao”) should be reserved for A. annua.34
(Other species in the genus Artemisia have historically been used to
treat malaria, including but not limited to A. absinthium and A.
abrotanum in Europe, A. afra in Africa, and A. argyi in
China.35)
In 1973,
artemisinin was altered to produce the semisynthetic derivative
dihydroartemisinin (DHA), from which other important and widely used
derivatives are produced, such as artesunate and artemether. “During evaluation
of the artemisinin compounds, we found that dihydroartemisinin was more stable
and ten times more effective than artemisinin,” Tu wrote. “More importantly,
there was much less disease recurrence during treatment with this derivative.”29
Furthermore, unlike artemisinin, DHA is water soluble.30
Solubility is
an important property of drugs, and one that often poses challenges to drug
formulators. Drugs that are hydrophobic have a low dissolution rate in the aqueous
gastrointestinal fluids when administered orally, resulting in reduced
bioavailability (the proportion of the administered amount of a drug that is
available at the site of physiological activity).36 On the other
hand, drugs that are extremely hydrophilic also are poorly absorbed because
they are unable to cross lipid-rich cell membranes.37
In the 1980s,
several thousand patients in China were successfully treated with artemisinin
and its derivatives, and news of their efficacy attracted worldwide attention.29,38
However, the WHO would not recommend the use of ACTs until April 2001, almost
30 years after artemisinin was identified. This hampered the efforts of aid
agencies, which could not buy drugs that were not approved by the WHO. Even
after the WHO’s recommendation, the drugs would not become widely available
until 2006, according to The New York Times.2,9
There were
several reasons for this delay. China’s isolationism certainly played a role.
In addition, under communism, patent law was nonexistent in China, and the
country took out no Western patents. This meant that anyone could use
artemisinin, which prevented pharmaceutical companies from being able to
exclusively produce and market the drug. There was also some general skepticism
about artemisinin, as there is with most new drugs. Whatever the reasons,
hundreds of thousands of African children were dying each year as artemisinin
idled, causing some to call the delay “genocidal.”2
The case of
artemisinin exemplifies how complex legal, economic, and political landscapes
can impede drugs from coming to market. It may also signal the need to minimize
these barriers to entry to allow people to receive the care they need.
Lasker-Debakey
Award and Nobel Prize
In 2011, the
prestigious Lasker-Debakey Clinical Medical Research Award was given to Tu by
the Lasker Foundation, which celebrates “the contributions of scientists,
clinicians, and public servants who have made major advances in the
understanding, diagnosis, treatment, cure, or prevention of human disease.”2,39
The Foundation named Tu “the discoverer of artemisinin,” which caused
controversy in the scientific community. Some said it was unfair to credit the
discovery to one individual, and named others they thought were equally
deserving, but Tu is widely credited with having had a major hand in almost all
of the events that led to the discovery.
This controversy
resurfaced in October 2015 when it was announced she would be awarded part of
the Nobel Prize in Physiology or Medicine. Tu, who, because of the nonexistent
patent laws in China at the time, has never financially benefitted from the
commercial use of artemisinin, said in a 2007 interview, “I do not want fame.
In our day, no essay was published under the author’s byline.”10,40
In fact, Tu was one of four anonymous authors of the original 1977 paper on
artemisinin.2
Shortly before
accepting the Nobel Prize in December 2015 in Stockholm, Sweden, Tu, 84 at the
time, responded to the controversy in an interview with The New York
Times: “Everyone is entitled to his opinion. We all believed in
collectivism. All I wanted was to do good work at my job. Of course, I’d be
nothing without my team. Foreign countries, like the United States, care a lot
about which individual should claim credit. Foreigners read historical records
and picked me. Chinese awards are always given to teams, but foreign awards are
different. This honor belongs to me, my team, and the entire nation,” she said.40
In a different
New York Times article, Tu is quoted as saying, “Artemisinin is a gift
for the world people from the traditional Chinese medicine.”41
Chemistry of
Artemisinin and Its Derivatives
Artemisinin
belongs to a class of compounds known as sesquiterpene lactones, which contain
15 carbon atoms (three isoprene units with five carbon atoms each) and a
lactone ring.
“Sesquiterpene
lactones come in different types of classes, with the class also defining the
stereochemistry of the molecules [i.e., the relative spatial arrangement of
atoms within the molecules],” said Eloy Rodriguez, PhD, the James A. Perkins
Endowed Professor of Environmental Toxicology and Medical Ethnopharmacognosy at
Cornell University and member of ABC’s Advisory Board (oral communication,
February 24, 2016). Rodriguez is an expert on this class of compounds, and has
identified 30 or 40 novel structures with his colleagues and students.
“Stereochemistry is very important in biological activity. … The degree of
oxygenation, or the degree of oxygens in the molecule, is [also] very important
in determining biological activity,” he said. He also said that these compounds
rarely contain nitrogen or chlorine and that they tend not to affect the
central nervous system.
“[Sesquiterpene
lactones have] been around for hundreds of millions of years,” Rodriguez said.
“And what makes the sunflower [Asteraceae] family so unique is the fact that it
makes this incredible array of sesquiterpene lactones.”
With more than
5,000 structures identified to date, sesquiterpene lactones are probably the
largest class of secondary metabolites found in plants. These compounds display
a wide range of biological activities, including antitumor, anti-inflammatory,
analgesic, antiulcer, antibacterial, antiviral, antifungal, insect deterrent,
and, of course, antiparasitic.33
“These
molecules evolved primarily as a defense, as insecticide, as repellent, against
herbivores, things that like to eat plants, or like to infect plants, such as
bacteria, fungi. So, these molecules, not only did they evolve, effectively, to
knock out enzymes in insects and other predators, it’s not surprising that
[some] also have the same effect against Plasmodium, because, as far as
the molecule is concerned, Plasmodium is just one big caterpillar inside
of your body. It kills it the way it would kill a caterpillar,” Rodriguez said.
According to
one source, artemisinin and its derivatives are the most potent and rapidly acting
antimalarial drugs ever discovered.35 They are highly active against
and most commonly used for infections of P. falciparum, the deadliest
species in humans, but some sources suggest they work as well, if not better,
against P. vivax, the most geographically widespread species.42,43
These drugs, however, do not affect all stages of the parasite’s life cycle
equally. They are inactive against the pre-liver stage (sporozoites) and liver
stages. (Since symptoms do not manifest until the blood stages, diagnosis at
this point is seemingly impossible anyway). In fact, they are inactive against
all extra-erythrocytic forms, which also includes merozoites. Late-stage ring
parasites and trophozoites are generally more vulnerable to artemisinin and its
derivatives than are schizonts or small rings.43,44
The inhibitory
effects of artemisinin and its derivatives against trophozoites prevent the
progression of the disease and reduce the formation of gametocytes, the dormant
sexual forms of the parasite.45 This is important because
eliminating gametocytes in the human host prevents the parasite’s life cycle
from restarting in the mosquito host, in the event that a female mosquito in
the genus Anopheles were to take a blood meal from the infected human.
Stage specificity is an important consideration with antimalarial drugs,
especially for patients with severe malaria. Since severe malaria is usually
fatal within 48 hours after symptoms present (i.e., the time it takes P.
falciparum, P. vivax, and P. ovale to complete one
asexual multiplication cycle within an infected erythrocyte), it is mainly the
parasites present at the time the patient presents for medical care that will
determine whether the patient lives or not.46
Artemisinin
and its derivatives are safe and well-tolerated. Some reported adverse effects
include mild gastrointestinal disturbances, dizziness, tinnitus (ringing in the
ears), and bradycardia (slow heart rate).42 The greatest concern
regarding these drugs is the neurotoxicity that has been reported in some
animal studies.45
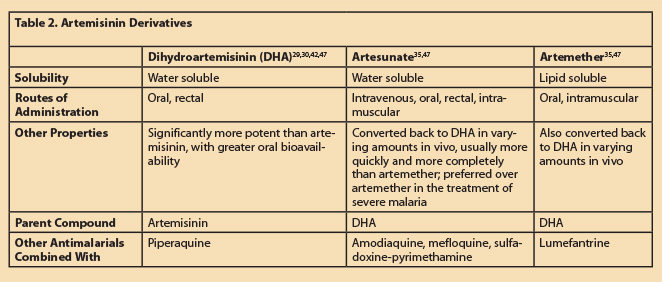
It should be
noted that artemisinin itself is not used as a component in any of the five
current WHO-recommended ACTs. This is primarily because of its poor solubility
in both water and oil, and because of its poor bioavailability. DHA,
artesunate, and artemether are all more potent and have greater oral
bioavailability (> 60%) than artemisinin.33,42 Furthermore, since
artesunate is more water soluble than other artemisinin derivatives, it can be
administered effectively intravenously. It can also be given orally, rectally,
or intramuscularly. Since artemether is lipid soluble, it can be administered
effectively intramuscularly or orally. Non-oral (i.e., parenteral)
administration is often necessary for patients with severe malaria, because
they are often unconscious or too ill to swallow.35
DHA is two- to
threefold more active than artemether. Artemether, however, is metabolized back
to DHA in varying amounts in vivo, depending on the route of administration
used. The same is true for artesunate, which is preferred over artemether in
the treatment of severe malaria. This is partly because after intramuscular
injection, artemether is often absorbed more slowly and erratically than
artesunate, which is absorbed quickly and reliably.47
Artemisinin
and its derivatives also have potent anticancer effects. They have been shown
to target a wide variety of cancer cells (including leukemia, breast, colon,
prostate, pancreas, ovarian, hepatic, renal, melanoma, osteosarcoma, central
nervous system, and lung cancer cells), with almost no negative effects on
healthy cells. In addition, DHA is active against other parasites, including Trichomonas
vaginalis and Giardia lamblia, as well as against species of the
genera Schistosoma, Toxoplasma, and Leishmania.33
Artemisinin-based
Combination Therapies
ACTs combine
DHA, artemether, or artesunate with another antimalarial drug that lasts longer
and has a different mode of action. The artemisinin component rapidly clears
the blood of the vast majority of parasites, while the partner drug eliminates
the remaining parasites. ACTs are generally administered over a three-day
treatment period.47
The three-day
course covers two of the parasite’s 48-hour intra-erythrocytic asexual cycles.47
The artemisinin component alone reduces parasite numbers by about 10,000-fold
in each cycle (compared to 100- to 1,000-fold for other antimalarial drugs35),
ensuring that only a tiny fraction of the parasites (< 0.0001% of those
present at the peak of the infection, according to one source42)
remain for the slowly eliminated partner drug to clear. This reduces the
potential for parasites to develop resistance to the partner drug, and the
partner drug reciprocally reduces the potential for parasites to develop
resistance to the artemisinin component.
ACTs are
recommended by the WHO as first-line treatment for uncomplicated P.
falciparum malaria.48 By April 2006, 60 countries had adopted
ACTs into their national treatment policies, primarily as first-line treatment,
and by the end of 2013, 79 countries had adopted them as first-line treatment
policy.9 The WHO recommends treating P. vivax infections with
chloroquine in areas where chloroquine is still effective. In areas with
chloroquine-resistant P. vivax, ACTs should be used (except for pregnant
women in their first trimester, who should be treated with quinine).47,48
In addition, adults and children with uncomplicated malaria caused by P.
malariae, P. ovale, or P. knowlesi should be treated with
either chloroquine (where effective) or an ACT.
For severe
malaria, the WHO recommends treating adults and children with intravenous or
intramuscular artesunate (or artemether, in preference to quinine, if
parenteral artesunate is unavailable) for at least 24 hours. Once the patient
is well enough to tolerate oral medication, treatment should be completed with
an ACT for three days.47
According to
the third edition of the WHO’s Guidelines for the Treatment of Malaria,
all five recommended ACTs have been shown to result in cure rates of >95% in
the absence of resistance.47 ACTs have also been reported to reduce
malaria mortality by 20-30% overall.3 Additionally, for
uncomplicated P. falciparum malaria, ACTs have been estimated to reduce
mortality in children aged one to 23 months by 99% (of the total who received
an ACT), and in children aged 24-59 months by 97%, according to the WHO’s World
Malaria Report 2015. Furthermore, in sub-Saharan Africa, parasite
prevalence among children aged two to 10 years is estimated to have decreased
from 33% in 2000 to 16% in 2015, and ACTs are estimated to have been
responsible for 14% of that reduction.17
Though the
primary purpose of ACTs is to avert severe disease and death, prompt treatment
can also reduce the incidence of uncomplicated cases. It is estimated that ACTs
averted 139.23 million cases of malaria in sub-Saharan Africa between 2001 and
2015. It is also estimated that, in sub-Saharan Africa, ACTs saved the public
sector about $156 million in health care costs between 2001 and 2014, based on
the number of cases that are estimated to have been averted during that time
period and the estimated number of those cases that would have sought care in
the public sector.
From 2005 to
2014, the number of ACT treatment courses procured from manufacturers increased
from 11 million to 337 million (almost a 3,000% increase). The WHO African
region accounted for almost 98% of manufacturer deliveries of ACTs in 2014.
Furthermore, in 2014, 223 million ACTs were delivered by manufacturers to the
public sector and 169 million ACTs (about 50% of those procured) were
distributed by national malaria control programs (NMCPs; i.e., domestic funding
mechanisms) through public sector facilities. International sources (including
aid organizations like the Global Fund to Fight AIDS, Tuberculosis and Malaria;
The United States President’s Malaria Initiative; The World Bank; and UNICEF)
spent $403 million on ACTs in 2014.
There are at
least three main reasons artemisinin derivatives are combined with partner
drugs. First, though they are the most effective of all antimalarials, they are
the most rapidly eliminated, with half-lives (i.e., the time it takes for half
of the administered amount of a drug to be eliminated from the bloodstream) on
the order of one hour.42 “You don’t need a long life for it to
work,” Rodriguez said. According to him, predators trying to consume the sweet
wormwood plant would have almost immediately been met head-on by artemisinin.
“I don’t think [the plant is] going to put that much energy into making a
molecule that’s going to be as solid as a rock,” he said. That being said, it
is estimated that for a three-day combination treatment course, the half-life
of at least one component should exceed 24 hours. Piperaquine, for example,
which is combined with DHA, has an estimated half-life of two to three weeks.42
Second,
artemisinin derivatives, when used as monotherapy (i.e., without a partner
drug), have relatively high recrudescence (i.e., relapse) rates of about 10%,
and they need to be administered over about seven days for radical cure.8
Third,
combination therapies prevent the development of resistance. “It’s kind of
difficult to develop resistance to multiple weapons, compared to one,”
Rodriguez said. “That’s always been my argument why, in the long run,
plant-derived mixtures work. The plant mixture might not be 100% effective,
like a pure compound, but it will be more difficult for bacteria or parasites
to develop resistance over a short period of time to a mixture.”
For this
reason, the WHO vehemently discourages the use of artemisinin monotherapies. In
January 2006, the WHO issued a press release urging pharmaceutical companies to
stop marketing and selling monotherapies. The press release cautioned that
once-popular antimalarials, including chloroquine and
sulfadoxine-pyrimethamine, became widely ineffective due to the development of
resistance.49
“Our biggest
concern right now is to treat patients with safe and effective medication and
to avoid the emergence of drug resistance. If we lose ACTs, we’ll no longer
have a cure for malaria, and it will probably be at least ten years before a
new one can be discovered,” Arata Kochi, PhD, the former director of the WHO’s
malaria department, is quoted as saying in the press release. (That was 10
years ago, and nothing more effective than ACTs has become available.)
By 2015,
artemisinin-resistant P. falciparum had been identified in Cambodia,
Laos, Myanmar, Thailand, and Vietnam.17 According to Rodriguez,
that’s not too surprising. “Some of them [the parasites] probably already were
resistant to it, but as more and more of the resistant strains take over the
population, then you have resistance,” he said. “[Plasmodium] is in a
battle, and it wants to live too. It doesn’t want to die, so resistance is
going to be around forever.” Encouragingly, as of November 2015, of the 78
national health authorities that need ACTs, 49 have taken regulatory measures
to withdraw the marketing authorization of oral monotherapies and 22 have never
registered them, leaving just seven that still allow the marketing of these
therapies.50
The five
current WHO-recommended ACTs are artemether/lumefantrine,
artesunate/amodiaquine, artesunate/mefloquine, DHA/piperaquine, and
artesunate/sulfadoxine-pyrimethamine.47 Artemether/lumefantrine,
known as Coartem (Novartis; Basel, Switzerland), was the first ACT and the one
that finally got the ball rolling in terms of making these drugs broadly
available.2
Factors to be
taken into consideration when choosing the appropriate ACT include local data
on the efficacy of the ACT, local data on drug resistance, the adverse effects
of the partner drug, availability, and cost.47
Sustainability
As with other
medicines derived from natural sources, there are challenges related to the
sustainable supply of artemisinin. First, A. annua generally yields low
quantities (between 0.01% and 0.80%) of the compound.51 Plants yielding
higher quantities are chosen for cultivation, but large amounts of dried plant
material still are required for relatively small amounts of artemisinin.
Long lead
times also contribute to the challenge. Artemisia annua takes about
eight months to reach full growth, at which point leaves are harvested and sent
to extraction facilities that usually rely on large numbers of small farmers
for their supply. In the past, China and Vietnam have accounted for about 80%
of the harvest volume of A. annua, while East Africa has accounted for
about 20%. After extraction, artemisinin is sent to specialized manufacturers
(sometimes the manufacturer of the finished product) to be converted into its
derivatives, and then the finished drug product is produced. The entire
process, from the planting of the seed to the finished product, takes about 14
months.52
The supply of
artemisinin has been erratic over the years. During shortages, prices
skyrocket, which causes more farmers to grow A. annua, and then the
supply increases greatly, depressing prices and causing another shortage.53
Consequently, artemisinin prices have fluctuated drastically, but there has
been an overall downward trend over time. Prices ranged from $800-$1,100 per
kilogram ($363-$499 per pound) in 2005, and from $270-$350 per kilogram
($122-$159 per pound) in 2013.54
From 2013 to
2014, the total number of ACT treatment courses procured from manufacturers
actually decreased from 392 million to 337 million.17,55 This is
partially because of increased efforts to diagnose malaria before administering
ACTs. In the past, patients with fevers were often treated with ACTs without
being diagnosed with malaria. Many of them did not actually have the disease.53
In fact, in sub-Saharan Africa, the number of diagnostic tests provided is now
greater than the number of ACTs distributed. This was not previously the case.
Despite the decrease in demand for ACTs from 2013 to 2014, between 68 and 80
million (74-87%) of the 92 million children with malaria in sub-Saharan Africa
did not receive an ACT in 2014, so there is a need to increase availability of
the drugs.17
Artemisia
annua is not the
only viable source of artemisinin. In 2004, the Bill and Melinda Gates
Foundation helped fund the development of a semisynthetic process of producing
the compound. The Foundation’s goal was to stabilize the supply of artemisinin
and lower the cost of each ACT treatment from $2.40 to “well under a dollar.”53
The method that was eventually developed involves genetically modified yeast,
which first converts glucose into artemisinic acid, a precursor to artemisinin.
Then, a process using light converts the acid into artemisinin. French
pharmaceutical company Sanofi has the capacity to produce between 50 and 60
tons of semisynthetic artemisinin per year using this method. That’s enough to
produce 125 million treatments.54 In addition, this method
drastically reduces the lead time to just a few days.52
However,
partially because of a plentiful supply and low prices of A. annua,
Sanofi reportedly produced no artemisinin using this method in 2015, and plans
to sell its manufacturing facility.53 Despite this, the potential to
quickly produce high-quality artemisinin that is not subject to seasonal and
other growing conditions and that is comparable in cost to naturally-occurring
artemisinin does exist.54
Conclusion
The discovery
of artemisinin by Tu Youyou and her team would seem to validate that the
ethnobotanical approach to drug discovery can be successful. In this case,
extensive study of the TCM literature helped produce the most effective drugs
ever discovered for treating one of the most devastating diseases in history:
malaria.
“The
ethnobotanical and ethnomedical roots of the development of artemisinin
demonstrate, beyond a doubt, both the profound history of traditional medicine
and the interface of traditional medicine and contemporary Western scientific
drug development,” said Steven King, PhD, senior vice president of
ethnobotanical research and sustainable supply at Jaguar Animal Health and
member of ABC’s Advisory Board (email, April 12, 2016).
King also said
that artemisinin “indicates that careful attention to the ethnobotanical detail
of how plant medicines are prepared can make all the difference in discovering
bioactive molecules that can become important therapies for global public
health. … If [Tu and her team] had not carefully studied the ethnobotanical
information, they might have given up on this plant and preparation.”
Beginning in
the 1990s, when King was at Shaman Pharmaceuticals Inc., he was part of a group
that looked for new drugs based on an ethnobotanical approach. Those efforts
eventually produced crofelemer, a natural compound isolated from the red latex
of the South American tree sangre de grado (dragon’s blood; Croton
lechleri, Euphorbiaceae).56 In 2012, crofelemer (trade name
Fulyzaq) became the second botanical, and the first orally administered botanical,
to receive drug approval from the US Food and Drug Administration (FDA). The
drug is used to treat HIV-associated diarrhea, and it demonstrates that, even
decades after the discovery of artemisinin, plants and other natural sources
should still be considered viable leads for new and effective drugs.
“The global
large- and small-scale pharmaceutical research approach has shifted away from
natural products and ethnobotanical information over the past 30 years,
focusing rather on high throughput screening, genomics, and related
approaches,” King said. The most often mentioned reason for this shift,
according to King, is that the chemical diversity found in plants has been
explored and hasn’t produced any new therapeutics. “This is not, by any means,
fully accurate, but microorganisms, marine compounds, and extremophiles
(organisms that thrive in extreme environments, such as hydrothermal vents in
ocean trenches) continue to be of interest in the search for new drugs. It
would be a wise idea to integrate the wisdom of traditional medicine with the
latest advances in drug discovery and development. There are so many examples
of new applications for ethnobotanically-derived therapeutics,” he said.
According to
King, the Nobel Prize reinforces “that plant medicine has been, and continues
to be, a critical part of the global management of human health. A plant-based
medicine does not have to become, or lead to, a new drug to demonstrate its
utility to human and animal health. … Plants as medicines are part of the
foundation of human health care worldwide, and will become more so in the 21st
century.”
He also said
that the Nobel Assembly’s recognition of Tu Youyou and artemisinin, as well as
its recognition of avermectin, is “timely and symptomatic of a scientific
community that is hopefully becoming more holistic and integrated.”
SIDEBAR In-Depth: Malaria
Malaria,
sometimes called the scourge of the tropics, has probably existed for hundreds
of thousands of years, likely predating modern humans.2,14 It is
thought that the first vertebrate hosts of the disease were reptiles.
In 400 BCE,
long before the term “malaria” was coined, Hippocrates wrote about the disease
in his treatise On Airs, Waters, and Places.15 And long
before that, a Chinese medical text, The Canon of Medicine, from 2700
BCE, described several characteristic symptoms of malaria.16 It was
not until 1880 that French army surgeon Charles Louis Alphonse Laveran
discovered the parasites that cause the disease in the blood of a patient. For
his discovery, Laveran was awarded the Nobel Prize in Physiology or Medicine in
1907.
The term
“malaria” is derived from the Italian mal’aria, a contracted form of mala
aria, meaning “bad air,” because the disease was once thought to be caused
by the foul, vaporous air of marshy areas. The term is thought to have first
been used by Italian historian Leonardo Bruni (circa 1370-1444).15
According
to the WHO’s World Malaria Report 2015, there were 95 countries and
territories with ongoing malaria transmission in 2015. This includes almost all
of Africa, almost all of the Middle East, almost all of Central and South
America, and most of Asia and Southeast Asia.17 Malaria was
eliminated from the United States in the early 1950s.18
In 2015,
there were about 214 million cases of malaria, an 18% decline from 2000 when
there were about 262 million cases. About 88% of the cases in 2015 occurred in
the WHO African region. In 2015, there were about 438,000 deaths from malaria
(an average of 1,200 deaths per day), a 48% decline from 2000 when there were
about 839,000 deaths. About 90% of the deaths in 2015 occurred in the WHO
African region. In 2015 about 306,000 deaths (70% of the total) were in
children under five years old. About 95% of these deaths occurred in the WHO
African region.17
Malaria in
humans is caused by five protozoan species in the genus Plasmodium: P.
falciparum, P. vivax, P. malariae, P. ovale, and P.
knowlesi (though it has been shown that P. knowlesi is not spread
from human to human like the other four species, but occurs when a mosquito
becomes infected after biting an infected monkey and then infects a human
[zoonotic transmission]).17 These primitive, unicellular protozoa
are eukaryotic, meaning that unlike bacteria, which are prokaryotic, they
contain membrane-bound organelles (e.g., a nucleus). And unlike viruses, which consist
of genetic material encapsulated in protein and are smaller than single cells,
these ancient, animal-like protozoa are considered living.19,20
The life
cycle of malaria parasites is fairly complex, and can be divided into two main
phases: the asexual cycle in humans and the sexual cycle in female mosquitoes
of the genus Anopheles. There are about 400 species in this genus, but
only 30 are significant to the transmission of malaria.17, 21-24
When an infected female, acting as a “vector,” bites a human, it injects saliva
to prevent the blood from clotting. From the mosquito’s saliva, the parasites
(called sporozoites at this stage) move into the bloodstream, and, within about
30 or 40 minutes, make their way to the liver, part of the body’s blood filter
system, where they invade liver cells (hepatocytes).
Over the
next 6 to 15 days, the parasites undergo asexual multiplication, copying their
DNA over and over again. A single parasite can multiply thousands of times in a
single hepatocyte. The specific molecular mechanisms that facilitate sporozoite
selection and infection of hepatocytes are not fully understood, but the
parasites avoid being overcome by white blood cells (leukocytes) and mature
into schizonts in this environment. The schizonts then rupture and release
daughter cells called merozoites, which are modified to infect red blood cells
(erythrocytes). In P. vivax and P. ovale, a dormant liver stage
(hypnozoites) can remain in the liver and cause relapse weeks, or even years,
later, when they enter the bloodstream.
After
infecting the erythrocytes, the parasites become young trophozoites (this is
called the ring stage because of the parasite’s morphology at this point). This
is the stage during which the parasite is absorbing nutrients from the host. As
the parasite gets larger, the ring shape disappears, and the parasite is then
known as a trophozoite. The trophozoites then undergo another round of asexual
multiplication and develop into schizonts. The infected erythrocytes then burst
and release the merozoites, which can then infect new erythrocytes and restart
the process, or, inexplicably, develop into gametocytes (a dormant sexual
stage).
When a
female Anopheles mosquito takes a blood meal from an infected person, it
becomes infected. Ingested parasites other than the gametocytes are digested in
the stomach of the mosquito, but the gametocytes mature into male and female
gametes. Male gametes fertilize female gametes, forming zygotes, which develop
into actively moving ookinetes that migrate to the outer lining of the
mosquito’s stomach, where they form cysts. Each cyst produces thousands of
sporozoites that then infest the mosquito’s salivary glands, thus starting the
life cycle over again.
Plasmodium
falciparum is
the species responsible for the majority of malaria deaths.17 It
typically has a shorter incubation period (the time before the first symptoms
present), can multiply rapidly in the blood, and causes severe malaria at least
partially by a property not shared by the other four species that cause the
disease in humans: sequestration, in which infected erythrocytes stick to the
endothelial cells of blood vessels, causing obstruction of the microcirculation
and the dysfunction of organs, typically the brain in cerebral malaria.25-27
Plasmodium vivax, however, is more widespread geographically than P.
falciparum because it can develop in the mosquito host at lower
temperatures and higher altitudes.17
It is
important to note that blood stage parasites are responsible for the symptoms
of malaria.23 Symptoms of uncomplicated malaria include fever,
chills, general malaise, sweats, headaches, nausea and vomiting, body aches,
increased respiratory rate, weakness, enlarged spleen, enlarged liver, and mild
jaundice. Symptoms of severe malaria include cerebral malaria (which can cause
impaired consciousness, seizures, coma, etc.), severe anemia, hemoglobinuria
(hemoglobin in the urine), acute respiratory distress syndrome (ARDS), low
blood pressure, acute kidney failure, excessive acidity in the blood and tissue
fluids, and hypoglycemia (low blood glucose).28
SIDEBAR
Artemisinin:
Mechanisms of Action
It is
believed that artemisinin’s effectiveness is due largely to its unique
endoperoxide bridge (i.e., two bonded oxygen atoms between two carbon atoms; C-O-O-C),
which is contained within a six-membered ring. “The oxygen-oxygen bond in the
endoperoxide bridge is somewhat stable, but not as strong as a carbon-carbon
bond. Nonetheless, the endoperoxide bridge in artemisinin is very active when
broken,” said Rodriguez. It is worth noting that artemisinin derivatives that
lack this feature show no antimalarial activity.44
It is
also believed that heme* is responsible for catalyzing the cleavage (breakage)
of the endoperoxide bridge.44 During the trophozoite stage (the
feeding stage) of the parasite’s life cycle (see previous sidebar), according
to one estimate, P. falciparum ingests and digests about 70% of the
hemoglobin (a protein that carries oxygen from the lungs to the body’s tissues)
in an infected red blood cell (erythrocyte) in just a few hours. Hemoglobin is
an important nutrient source for the parasite and enables its growth and
maturation. As the parasite breaks down the hemoglobin, heme is released.57,58
When
the endoperoxide bridge is cleaved in the presence of ferrous iron from heme,
each of the previously bonded oxygen atoms retains one of the two previously
shared electrons (i.e., homolytic fission) and becomes a free radical (a highly
reactive, short-lived atom, or group of atoms, with one or more unpaired
electrons).44,59 The unstable compound then damages the
microorganelles and membranes of the parasite, as well as the infected
erythrocyte, causing the host’s immune system to eliminate the infected
erythrocyte. The theory that free radicals mediate the death of the parasites
is supported by the fact that the presence of antioxidants (free radical
scavengers) blocks the antimalarial effects of artemisinin.44
“You
can imagine it like a dart sticking to a dartboard,” Rodriguez said. “In other
words, the dartboard, in this case, could be a protein, an enzyme, and the dart
is the small molecule that just jams that board, or that protein, and then it
doesn’t function. … It’s always been a battle of small molecules against
macromolecules.”
He
proposed another explanation for artemisinin’s effectiveness. “We’ve done some
preliminary, but unpublished, research in which we show that artemisinin is
capable of cleaving DNA,” he said. “In other words, artemisinin can remove a
proton or a hydrogen from DNA that can lead to the eventual breakdown of DNA. …
If you have all these radicals just bombarding the DNA, it really messes it
up.”
*Heme
is a non-protein constituent of hemoglobin that contains, at its center, a
ferrous iron atom (i.e., an iron atom with two more protons than electrons; Fe2+).
References
- Perlez J. Answering an Appeal by Mao Led Tu Youyou, a Chinese Scientist, to a Nobel Prize. New York Times. October 6, 2015. Available at: www.nytimes.com/2015/10/07/world/asia/tu-youyou-chinese-scientist-nobel-prize.html?_r=1. Accessed February 25, 2016.
- McNeil DG Jr. For Intrigue, Malaria Drug Gets the Prize. New York Times. January 16, 2012. Available at: www.nytimes.com/2012/01/17/health/for-intrigue-malaria-drug-artemisinin-gets-the-prize.html. Accessed February 25, 2016.
- The 2015 Nobel Prize in Physiology or Medicine. Nobel Prize website. October 5, 2015. Available at: www.nobelprize.org/nobel_prizes/medicine/laureates/2015/press.html. Accessed February 25, 2016.
- Johnson I. Nobel Renews Debate on Chinese Medicine. New York Times. October 10, 2015. Available at: www.nytimes.com/2015/10/11/world/asia/nobel-renews-debate-on-chinese-medicine.html?_r=0. Accessed February 25, 2016.
- Cechinel-Filho V, ed. Plant Bioactives and Drug Discovery: Principles, Practice, and Perspective. Hoboken, NJ: John Wiley & Sons, Inc.; 2012.
- Lew K. Mosquito-borne Illnesses. Tarrytown, NY: Marshall Cavendish; 2009.
- Staines HM, Krishna S, eds. Treatment and Prevention of Malaria: Antimalarial Drug Chemistry, Action and Use. New York, NY: Springer Science and Business Media; 2012.
- Maude RJ, Woodrow CJ, White LJ. Artemisinin antimalarials: Preserving the “magic bullet.” Drug Dev Res. 2010;71(1):12-19. doi: 10.1002/ddr.20344.
- WHO Briefing on Malaria Treatment Guidelines and artemisinin monotherapies. WHO website. Available at: www.who.int/malaria/publications/atoz/meeting_briefing19april.pdf. Accessed March 10, 2016.
- Phillips T. Tu Youyou: How Mao’s challenge to malaria pioneer led to Nobel Prize. The Guardian. October 5, 2015. Available at: www.theguardian.com/science/2015/oct/05/youyou-tu-how-maos-challenge-to-malaria-pioneer-led-to-nobel-prize. Accessed March 11, 2016.
- Appendix A—Description of Antimalarial Drugs. PubMed website. Available at: www.ncbi.nlm.nih.gov/books/NBK221160/. Accessed March 11, 2016.
- Miller LH, Xinzhuan S. Artemisinin: Discovery from the Chinese Herbal Garden. Cell website. Available at: www.cell.com/cell/fulltext/S0092-8674(11)00950-0. Accessed March 8, 2016.
- Willcox M, Bodeker G, Rasoanaivo P, eds. Traditional Medicinal Plants and Malaria. Boca Raton, FL: CRC Press; 2004.
- An ancient killer: ancestral malarial organisms traced to age of dinosaurs. Oregon State University website. March 25, 2016. Available at: http://oregonstate.edu/ua/ncs/archives/2016/mar/ancient-killer-ancestral-malarial-organisms-traced-age-dinosaurs. Accessed April 11, 2016.
- Hempelmann E, Krafts K. Bad Air, Amulets and Mosquitoes. Malar J. 2013;12:232. doi: 10.1186/1475-2875-12-232.
- The History of Malaria, an Ancient Disease. CDC website. Available at: www.cdc.gov/malaria/about/history/. Accessed March 19, 2016.
- World Health Organization. World Malaria Report 2015. WHO website. Available at: http://apps.who.int/iris/bitstream/10665/200018/1/9789241565158_eng.pdf?ua=1. Accessed March 20, 2016.
- Malaria Facts. CDC website. Available at: www.cdc.gov/malaria/about/facts.html. Accessed March 20, 2016.
- Germs: Understand and protect against bacteria, viruses and infection. Mayo Clinic website. Available at: www.mayoclinic.org/germs/art-20045289. Accessed March 20, 2016.
- Eukaryotic Cell vs. Prokaryotic Cell. Diffen website. Available at: www.diffen.com/difference/Eukaryotic_Cell_vs_Prokaryotic_Cell. Accessed March 20, 2016.
- Critchlow A, Staves J, Watt C. Malaria Vaccines. Stanford website. Available at: http://web.stanford.edu/class/humbio153/MalariaVac/index.html. Accessed March 21, 2016.
- The Malaria Life Cycle Explained. YouTube website. Available at: www.youtube.com/watch?v=WoIO-g1hiSo. Accessed March 21, 2016.
- Malaria Biology. CDC website. Available at: www.cdc.gov/malaria/about/biology/. Accessed March 21, 2016.
- Malaria. Tulane website. Available at: www.tulane.edu/~wiser/protozoology/notes/malaria.html. Accessed March 28, 2016.
- Malaria Parasites. CDC website. Available at: www.cdc.gov/malaria/about/biology/parasites.html. Accessed March 21, 2016.
- Plasmodium Falciparum. Scientists Against Malaria website. Available at: http://scientistsagainstmalaria.net/parasite/plasmodium-falciparum. Accessed March 21, 2016.
- Berendt AR, Ferguson DJP, Newbold CI. Sequestration in Plasmodium falciparum malaria: Sticky cells and sticky problems. Parasitology Today. 1990;6(8):247-254. doi: 10.1016/0169-4758(90)90184-6.
- Malaria Disease. CDC website. Available at: www.cdc.gov/malaria/about/disease.html. Accessed March 21, 2016.
- Tu Y. The discovery of artemisinin (qinghaosu) and gifts from Chinese medicine. Nature Medicine. 2011;17:1217-1220. doi: 10.1038/nm.2471.
- Hsu E. Reflections on the ‘discovery’ of the antimalarial qinghao. Br J Clin Pharmacol. 2006;61(6):666-670. doi: 10.1111/j.1365-2125.2006.02673.x
- Prescriptions for Fifty-two Diseases (Wu Shi Er Bing Fang). AT0086 website. Available at: http://news.at0086.com/Chinese-Medicine/Wu-Shi-Er-Bing-Fang-Prescriptions-for-Fifty-two-D.html. Accessed March 12, 2016.
- Which is the best solvent for herbal extraction? ResearchGate website. Available at: www.researchgate.net/post/Which_is_the_best_solvent_for_herbal_extraction. Accessed March 12, 2016.
- Ivanescu B, Miron A, Corciova A. Sesquiterpene lactones from Artemisia genus: biological activities and methods of analysis. J Anal Methods Chem. 2015;2015:247685. doi: 10.1155/2015/247685.
- Hsu E, Harris S. Plants, Health and Healing: On the Interface of Ethnobotany and Medical Anthropology. New York, NY: Berghahn Books; 2010.
- Willcox M. Artemisia Species: From Traditional Medicines to Modern Antimalarials — and Back Again. EnCognitive website. Available at: www.encognitive.com/files/Artemisia%20Species:%20From%20Traditional%20Medicines%20to%20Modern%20Antimalarials%E2%80%94and%20Back%20Again.pdf. Accessed March 28, 2016.
- Savjani K, Gajjar AK, Savjani JK. Drug Solubility: Importance and Enhancement Techniques. ISRN Pharm. 2012;2012:195727. doi: 10.5402/2012/195727.
- Clinical Pharmacology. University of Baghdad website. Available at: www.codental.uobaghdad.edu.iq/uploads/lectures/Pharma%20lectures/2%20Pharmacokinetics%20finishing%20with%20bioavailibility.pdf. Accessed March 16, 2016.
- YouYou Tu: Discovery of Artemisinin — A gift from Traditional Chinese Medicine to the World. YouTube website. Available at: www.youtube.com/watch?v=ZYuv2bFLTug. Accessed March 21, 2016.
- About the Foundation. Albert and Mary Lasker Foundation website. Available at: www.laskerfoundation.org/about/. Accessed March 21, 2016.
- Perlez J. Q and A: Tu Youyou on Being Awarded the Nobel Prize. Sinosphere website. October 9, 2015. Available at: http://sinosphere.blogs.nytimes.com/2015/10/09/tu-youyou-nobel-prize-malaria/. Accessed March 21, 2016.
- Buckley C. Some Surprise, and Affirmation, in China After Tu Youyou Receives Nobel Prize. Sinosphere website. October 6, 2015. Available at: http://sinosphere.blogs.nytimes.com/2015/10/06/nobel-china-medicine-tu-youyou-prize. Accessed March 21, 2016.
- Nosten F, White NJ. Artemisinin-based combination treatment based combination treatment of malaria.falciparum malaria. In: Breman JG, Alilio MS, White NJ, eds. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77(6) of American Journal of Tropical Medicine and Hygiene. Northbrook, Illinois: American Society of Tropical Medicine and Hygiene; December 2007. Available at: www.ncbi.nlm.nih.gov/books/NBK1713/. Accessed May 5, 2016.
- Artemisinin Derivatives: Summary of Nonclinical Safety Data Introductory Remarks. WHO website. Available at: http://apps.who.int/prequal/info_applicants/Guidelines/Nonclinical_Overview_Artemisinin-Derivatives.pdf. Accessed March 28, 2016.
- Meshnick SR, Taylor TE, Kamchonwongpaisan S. Artemisinin and the antimalarial endoperoxides: From herbal remedy to targeted chemotherapy. Microbiological Reviews. 1996;60(2):301-315. Available at: http://mmbr.asm.org/content/60/2/301.full.pdf. Accessed March 25, 2016.
- Antimalarial Drugs. Malaria Site website. Available at: www.malariasite.com/malaria-drugs/. Accessed March 28, 2016.
- White NJ. Antimalarial drug resistance. J Clin Invest. 2004;113(8):1084-1092. doi: 10.1172/JCI200421682.
- Guidelines for the Treatment of Malaria. Third Edition. WHO website. Available at: http://apps.who.int/iris/bitstream/10665/162441/1/9789241549127_eng.pdf?ua=1&ua=1. Accessed March 29, 2016.
- Overview of Malaria Treatment. WHO website. Available at: www.who.int/malaria/areas/treatment/overview/en/. Accessed March 29, 2016.
- WHO calls for an immediate halt to provision of single-drug artemisinin malaria pills. WHO website. January 19, 2006. Available at: www.who.int/mediacentre/news/releases/2006/pr02/en/. Accessed March 30, 2016.
- Marketing of oral artemisinin-based monotherapy medicines at country level. WHO website. Available at: www.who.int/malaria/monotherapy_NDRAs.pdf?ua=1. Accessed March 31, 2016.
- Pani A, Mahapatra RK, Behera N, Naik PK. Computational identification of sweet wormwood (Artemisia annua) microRNA and their mRNA targets. Genomics Proteomics Bioinformatics. 2011;9(6):200-210. doi: 10.1016/S1672-0229(11)60023-5.
- Shretta R, Yadav P. Stabilizing supply of artemisinin and artemisinin-based combination therapy in an era of wide-spread scale-up. Malaria Journal. 2012;11:399. Available at: http://malariajournal.biomedcentral.com/articles/10.1186/1475-2875-11-399. Accessed April 1, 2016.
- Peplow M. Synthetic Biology’s First Malaria Drug Meets Market Resistance. Scientific American. February 25, 2016. Available at: www.scientificamerican.com/article/synthetic-biology-s-first-malaria-drug-meets-market-resistance/. Accessed April 1, 2016.
- Stabilizing the antimalarial drug supply: Semisynthetic artemisinin could meet up to one-third of global need. PATH website. Available at: www.path.org/publications/files/DRG_ssart_fs.pdf. April 1, 2016.
- World Health Organization. World Malaria Report 2014. WHO website. Available at: www.who.int/m
- FDA approves Crofelemer as first-ever oral botanical drug [press release]. Austin, TX: American Botanical Council; January 2, 2013. Available at: http://cms.herbalgram.org/press/2013/FDA_Approves_Crofelemer.html. Accessed April 13, 2016.
- Goldberg DE, Slater AFG, Beavis R, Chait B, Cerami A, Henderson GB. Hemoglobin Degradation in the Human Malaria Pathogen Plasmodium falciparum: A Catabolic Pathway Initiated by a Specific Aspartic Protease. Rockefeller University website. Available at: http://lab.rockefeller.edu/chait/pdf/91/91_goldberg_j-exp-med.pdf. Accessed March 25, 2016.
- Lew VL, Tiffert T, Ginsburg H. Excess hemoglobin digestion and the osmotic stability of Plasmodium falciparum-infected red blood cells. Blood Journal. 2003;101(10). Available at: www.bloodjournal.org/content/101/10/4189. Accessed March 25, 2016.
- Basic principles in organic chemistry: Bond fission. Padakshep website. Available at: http://padakshep.org/otp/subjects/chemistry/organic-chemistry/bond-fission/. Accessed March 28, 2016.
|